Emerging Structural Shift in Health Futures: The Rising Foothold of Telehealth Peptide Prescription as a Regulatory and Market Inflection Point
This paper identifies the nascent yet under-recognized potential of telehealth-delivered peptide prescribing as a structural inflection in health futures. The signal intersects with regulatory relaxation, digital health expansion, and shifting insurance landscapes, promising to realign capital flows, regulatory oversight, and industrial incumbency over the next decade.
The convergence of telehealth normalization with peptide therapeutics — biologically active short chains of amino acids used for a variety of health conditions — forms a subtle but substantive disruptive inflection. Unlike more visible telehealth trends limited to mental health or primary care triage, peptide teleprescription embodies a complex regulatory gamble, poised to recalibrate pharmaceutical supply models, payer frameworks, and frontline digital health ecosystems. Its rise could scale into a paradigm-level transformation with implications spanning Asia Pacific aging populations to U.S. market privatization pressures.
Signal Identification
This development qualifies as an emerging inflection indicator with medium-to-high plausibility over a 5–10 year horizon. It is neither a widely debated wildcard nor a common weak signal, but a quietly scaling intersection of regulatory easing (especially by the U.S. Food and Drug Administration), telehealth infrastructure, and shifting insurance models affecting access to weight loss and chronic condition medications.
Sectors exposed include telehealth providers, pharmaceutical manufacturing and distribution, regulatory agencies, healthcare insurers, and chronic disease management services spanning the Asia Pacific and North American markets.
What Is Changing
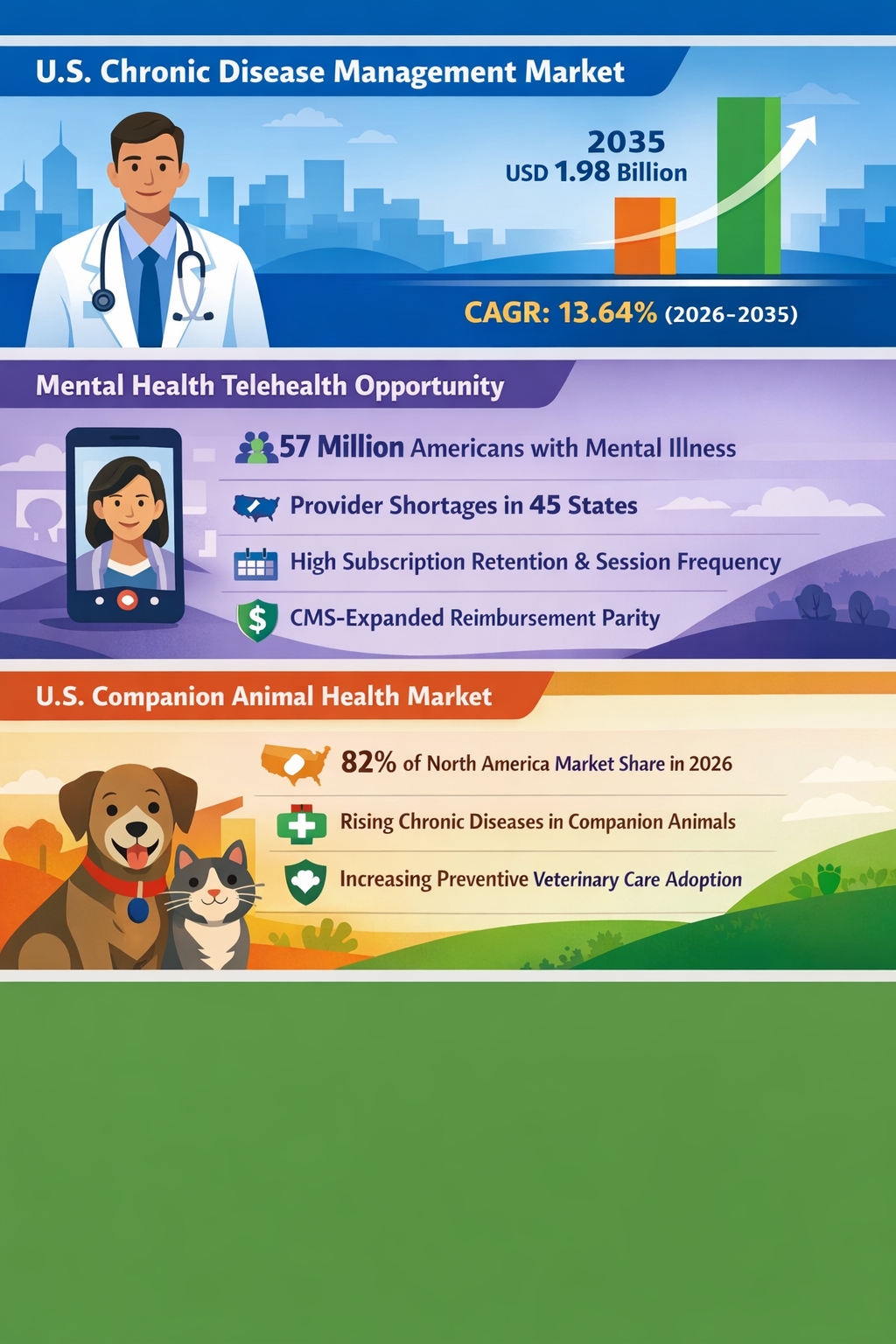
The Asia Health Fund’s focus on telehealth and underserved healthcare needs signals a broad structural shift toward digital intervention models targeting women’s and children’s health, anticipating growing demand in aging Asia Pacific regions with chronic disease burdens (The Asia Health Fund SSIR 01/01/2024); (Asia Pacific Regenerative Market Persistence Market Research 15/02/2024). This aligns with projected growth in telehealth utilization and infrastructure expansion to manage chronic illness efficiently, especially in cost-sensitive aging economies like Japan (Persistence Market Research 15/02/2024). Telehealth mental health services, a recognized immediate growth driver in North America, have benefited from Centers for Medicare & Medicaid Services (CMS) reimbursement parity expansions, highlighting a precedent for regulatory agility alongside digitization (Persistence Market Research 22/01/2024). However, peptide prescribing via telehealth remains a less observed but rapidly emergent phenomenon.
Telehealth peptide prescribing — forecast to potentially reach $2.2 billion annually in the near future — represents a novel digital pharmaceutical distribution vector, dependent on regulatory recalibration. Key players like Hims & Hers could capture significant market share if FDA restrictions on peptides ease, creating an alternative channel for consumer drug access outside traditional brick-and-mortar and pharmacy models (The Guardian 26/06/2026). Notably, this expansion coincides with employers increasingly dropping insurance coverage for expensive weight loss drugs such as Wegovy and Zepbound, further incentivizing telehealth providers to fill these coverage gaps (Scripps News 10/04/2024).
While telehealth for mental health is an acknowledged growth market, peptide prescribing is less visible but structurally different because it challenges the traditional pharmaceutical distribution system, introduces complex supply chain governance issues, and can disrupt insurer-provider-patient dynamics by circumventing conventional approval and coverage models.
Disruption Pathway
The signal could escalate under conditions of progressive regulatory openness towards peptide prescriptions via telehealth platforms. Successful CMS or FDA pilot policy adaptations that establish reimbursement parity and safety monitoring frameworks would accelerate adoption. Concurrently, worsening insurance coverage gaps for weight loss and chronic disease drugs amplify patient demand for digital alternatives, increasing telehealth peptide service uptake.
The emergent stresses would include regulatory challenges in managing quality assurance, potential diversion or misuse of peptide drugs, and pressure on legacy pharmaceutical distribution networks reliant on traditional prescriber-pharmacy models. Healthcare payers may face new liability frameworks as digital-first providers dispense biologics remotely without usual oversight, pushing regulators to innovate governance models emphasizing real-time data and digital authentication over legacy controls.
Structural adaptations might involve integrated telehealth-specialty pharma supply chains, creation of new digital formulary standards, and growth of decentralized compliance technologies such as blockchain-enabled prescriptions. Feedback loops, such as improved adherence driven by telehealth convenience boosting long-term outcomes, could validate the model, while negative externalities like increased illicit peptide markets might provoke iterative regulatory tightening or carve-outs.
Dominant incumbents in pharmaceutical distribution and health insurance may face existential pressures, catalyzing either strategic partnerships with telehealth disruptors or attempts to reassert control through regulatory capture or innovation in their own digital capabilities.
Why This Matters
For capital allocators, telehealth peptide prescription unveils an emergent investment avenue deviating from typical mental health or primary care telehealth plays, potentially shifting billions towards biologics-focused digital health ventures and vertically integrated pharma-supply startups. Regulators will need to reconsider frameworks around pharmaceutical safety standards, reimbursement parity, and cross-jurisdictional credentialing.
Competitively, traditional pharmaceutical distributors and brick-and-mortar pharmacies may lose market share unless they adapt or consolidate. Health insurers may encounter new forms of risk and cost exposure as coverage gaps drive telehealth uptake outside established networks. Supply chains will evolve toward demand-driven, digitally traceable biologic delivery systems, reconfiguring manufacturing, procurement, and fulfillment logistics.
Governance implications include evolving liabilities around digital prescribing, patient data protection, and potential policymaker reliance on real-world evidence generated from telehealth platforms to inform ongoing regulation.
Implications
This signal may scale into a foundational structural realignment of digital health markets by altering pharmaceutical dispensing and payer models. It could not be dismissed as transitory hype given the reinforcing dynamics of regulatory easing and insurance withdrawal from coverage of costly peptides.
However, the causal pathways are contingent on sustained regulatory agility and patient adoption overcoming trust barriers inherent in remote biologic therapy management. It is not merely an incremental telehealth expansion but a qualitative shift in how complex medicines reach consumers and how safety is monitored.
Competing interpretations include skepticism about the enforceability of digital prescriptions for peptides or regulatory backlash curbing telehealth pharmaceutical expansion due to safety concerns.
Early Indicators to Monitor
- FDA and CMS regulatory drafts or pilot programs enabling telehealth peptide prescribing and reimbursement parity
- Venture capital clustering around telehealth platforms specializing in peptide therapeutics or biologic prescription services
- Procurement shifts in pharmaceutical supply chains incorporating direct-to-consumer telehealth distribution channels
- Increased patent filings or standards formation around digital prescription authentication and biologics tracking
- Employer insurance policies increasingly dropping coverage for injectable weight loss and peptide therapies
Disconfirming Signals
- Regulatory reversals or stifling restrictions reinstating strict controls on peptide teleprescriptions
- Robust re-expansion of insurance coverage for peptide weight loss drugs mitigating demand shifts to telehealth
- Significant safety incidents or adverse outcomes linked to telehealth peptide prescribing triggering regulatory clampdowns
- Entrenched pharmaceutical distributors successfully lobbying for restrictive digital prescribing laws
Strategic Questions
- How should regulatory agencies balance safety oversight with innovation enabling telehealth peptide prescribing?
- What operational and partnership models can incumbents adopt to compete or collaborate with emerging telehealth peptide platforms?
Keywords
Telehealth; Peptide Prescription; Regulatory Innovation; Digital Pharmaceutical Distribution; Insurance Coverage; Chronic Disease Management; Capital Allocation
Bibliography
- The Asia Health Fund will target telehealth, nutrition, frontline health worker training, and underserved health needs of women and children. SSIR. Published 01/01/2024.
- Fastest-growing Region: Asia Pacific is projected to be the fastest-growing, driven by expanding healthcare infrastructure, rising surgical volumes, broader insurance coverage, and increasing chronic disease-related wound care demand. Persistence Market Research. Published 15/02/2024.
- Mental health telehealth represents the most time-sensitive actionable opportunity with 57 million Americans living with mental illness (SAMHSA) and 45 states reporting provider shortages, offering above-average subscription retention, high session frequency, and CMS-expanded reimbursement parity. Persistence Market Research. Published 22/01/2024.
- Telehealth peptide prescribing could reach $2.2bn per year, with Hims & Hers alone capturing as much as $440m if restrictions are eased. The Guardian. Published 26/06/2026.
- Telehealth providers like Hims and Hers could soon see more business, now that more and more employees are losing insurance coverage for weight loss drugs like Wegovy and Zepbound. Scripps News. Published 10/04/2024.
- Japan is expected to account for a 26% share of the Asia Pacific revenue in 2026 due to a rapidly aging demographic profile demanding cost-efficient chronic disease management models. Persistence Market Research. Published 15/02/2024.